



ABERDEEN PROVING GROUND, Md. (Sept. 19, 2012) -- The U.S. Army explored whether real-time, electronic point-of-treatment care was possible or practical this summer at its integrated capabilities testbed at Fort Dix, N.J.
Key medical and technical personnel from the U.S. Army Medical Research & Materiel Command and the U.S. Army Research, Development and Engineering Command combined prototype medical military software with commercial hand-held technologies and tactical 4G networks to send medical information from the point of injury on the battlefield back to the doctor for real-time communication and decision making.
"It's going to build confidence in the medic on the field that's isolated with a severely wounded Soldier," said Carl Manemeit, Physiological Monitoring project lead for the MRMC's Telemedicine & Advanced Technology Research Center, or TATRC.
"If you've ever seen the movie, 'Black Hawk Down,' the medic is trying to treat the guy with the artery issue in his leg; the medic goes through all his resources, and once he exhausted all his knowledge, he was stuck," Manemeit said. If he had been connected to the surgeons back at the treatment facility, they could have given him more guidance on how to save that Soldier's life. By injecting this expertise, we might be able to do that one thing that could save some guy's life; that's what we're looking to do."
Medics utilized man-portable physiological monitoring devices with streaming video, voice and photo capability, and sent electronic Tactical Casualty Care Cards, or TC3, over a tactical network to the surgical facility so surgeons could see injuries and what treatment had been performed prior to the patient's arrival.
"There's an information gap that lies between the point of injury on the field and point of treatment back at a medical facility," said Dr. Gary R. Gilbert, TATRC Research, Development, Test and Evaluation program manager for Secure Telemedicine. "We need to do a better job of being able to record what the medic saw and did prior to the patient being evacuated to the treatment facility, and we want this record to be transmitted to the Soldier's permanent health records."
"Now when the patient goes to a combat support hospital, or gets back to Walter Reed for further care, the doctors can see what happened in the field; and five years from now when the patient goes into a VA hospital seeking treatment, the care providers can see everything that's been done," Gilbert said.
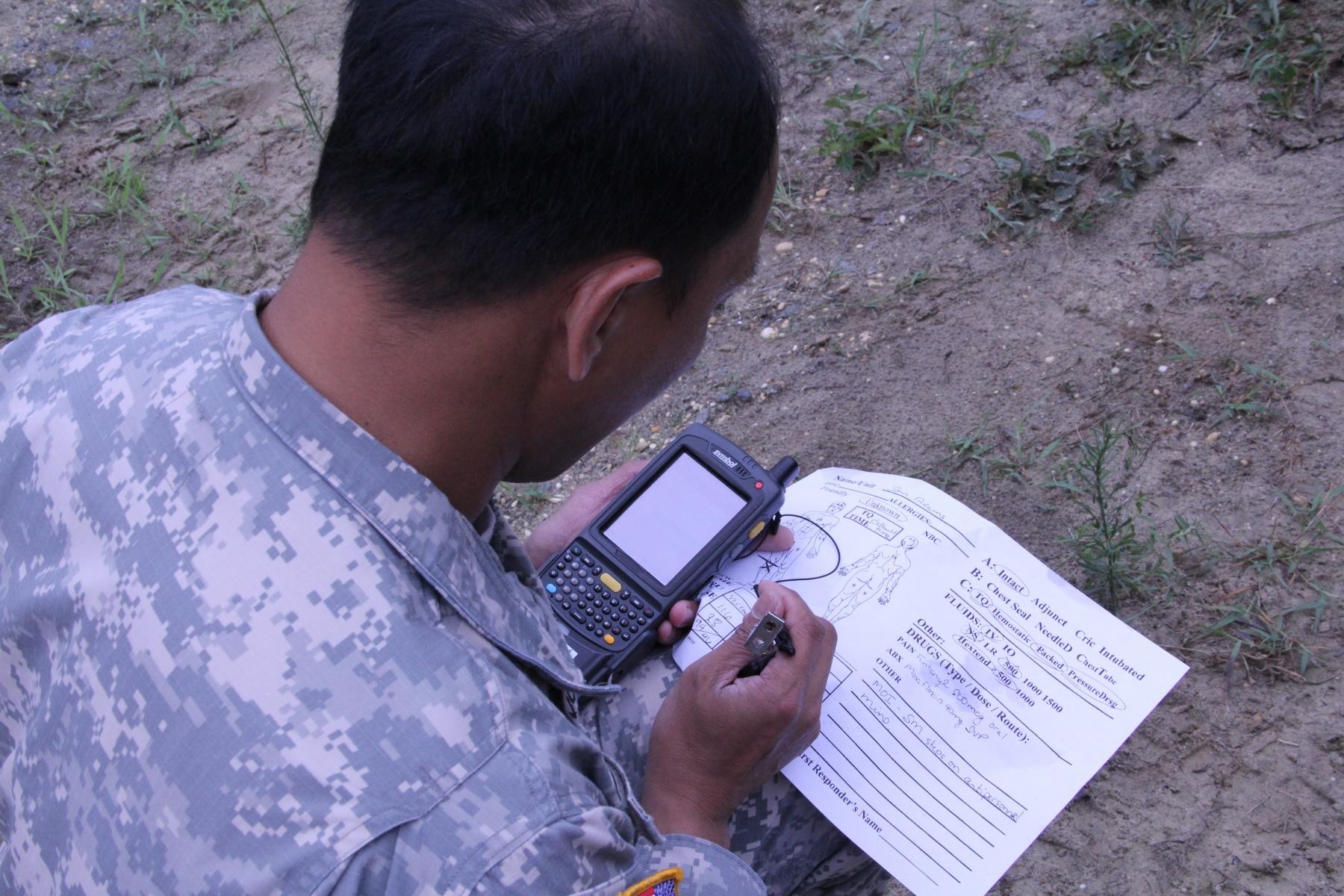
Currently, medics fill out a paper TC3 that's attached to the injured Soldier before evacuation to the battalion aid station or the combat support hospital. In some cases, the TC3 never makes it back to the treatment facility, and the information never makes it to the patient records.
"One of the issues I had with the card is that it's a piece of paper held on with a metal wire," said Spc. Daniel Vita, U.S. Army Medical Research Institute for Infectious Diseases, Fort Detrick, Md. "Pretty much, you would have attached it to the patient through his zipper or around his wrist, but you potentially had the problem of ripping the paper from the metal loop."
Vita, who was a medic with the 130th Engineer Brigade Headquarters in Iraq, preferred using tape and a sharpie because "it stayed."
"I like the idea of an electronic TC3 because it's simpler," Vita said. "It's a lot easier for the information to get to where it needs to go and it makes it legible. When you filled out a TC3 card and put it on the patient, they didn't know what was happening until that patient and card got to them. Now doing it electronically, you can send it ahead to the level two or three so they have an idea of what kinds of patients and casualties are coming in."
The combination of secure tactical communications and knowledge management may also help brigade surgeons prioritize treatment and evacuation assets so the most critically injured can be treated first.
"The Army uses medevac, but the bad news is that it costs about $20,000 per patient flight," said Dave Williams, Project Manager for Theater Tele-Health Initiatives, TATRC. "And if you have six assets and 12 patients, who should they get first? If we can determine which patients can be held and which can be treated and stabilized on site, it might be a less expensive way to save a patient's life."
The work was performed at the integrated capabilities testbed operated by Product Director Command, Control, Communications, Computers, Intelligence, Surveillance, Reconnaissance and Network Modernization, an R&D program within U.S. Army RDECOM's communications-electronics RD&E center, CERDEC.
"This is a forgiving environment because it's designed for testing and solution proving," Gilbert said. "If things don't work, that's OK; you find out what doesn't work and you fix it here. There are a lot of technologies required to make this work, and we don't have all of these. CERDEC is helping to fill in those gaps by providing a variety of radio capabilities that you wouldn't get at a real brigade: SRW, WNW, ANW2, deployable 4G, Airborne relay, connection to Army WIN-T. They provide the infrastructure, and we just bring the application."
PD C4ISR & Network Modernization focuses on the future network, near-term and several years out, providing the Army with a relevant venue to assess next-generation technologies and to facilitate technology maturation. The program is also a key component in CERDEC's support of the agile acquisition process, utilizing its field lab environment to perform risk mitigation and candidate assessment/selection for future Network Integration Rehearsal/Exercise events.
"These guys are not only preparing the current force to be successful, they're closing the gaps for the future force with each iteration of these integrated capabilities events," Williams said. "You don't solve all the problems in one 12-month cycle. This venue is providing the medics an opportunity to get inside the Program Objective Memorandum cycle to come up with those solutions and iteratively solve them as technologies emerge and grow with us. This has been a complete team effort to develop a solution that did not exist six years ago."
This is the third year that PD C4ISR & Network Modernization has examined network capabilities that could support the medic/first responder's mission.
During 2011, PD C4ISR & Network Modernization combined fielded tactical radios such as the Enhanced Position Location Reporting System with the Soldier Radio Waveform to see if it was possible and feasible to provide enhanced bandwidth and over-the-horizon communications for hand-held medical data. This year, a 4G cellular mesh network was implemented, using SRW to bridge back to the tactical network.
"We're examining how best to combine the future and current so we can enable the medical community to perform their mission more efficiently," said Jason Sypniewski, chief for PD C4ISR & Network Modernization's Integrated Event Design & Analysis branch. "We're looking at the Soldier Radio Waveform because it's a self-healing waveform that allows non-line-of-sight communication; that's the vision for where the Army wants to go. We've looked at EPLRS because it's an existing asset on which the medical community might could recapitalize."
"Cellular technology could be the future of tele-health on the modern battlefield, but we need to know if it can be done, and if so, would it actually enhance the delivery of information?" Sypniewski said. "As decision makers look at network modernization, this is the type of information they will want in order to help them make informed decisions regarding telemedicine capabilities and the networks on which they're going to ride. Our mission is to provide this."
Related Links:
U.S. Army Research, Development and Engineering Command
Communications-Electronics Research, Development and Engineering Center
Social Sharing