
The 1.13 million square-foot Fort Bliss Hospital Replacement Project in El Paso, Texas, is a military construction program intended to replace the 40-year-old William Beaumont Army Medical Center at a cost of $1.3 billion. The project acquisition method used was the design-bid-build method, in which construction follows a complete design or 100 percent design effort. The six-building secure campus consists of a main hospital, outpatient clinics, administrative building, clinical investigation (research) facility, central utility plant, a visitor control center and two access control points. It is scheduled to be open Sept. 30.
As the Fort Bliss Hospital Replacement Project was approaching its substantial completion phase, the U.S. Army Health Facility Planning Agency project office was looking for targets of opportunity before construction completion to expedite the initial outfitting and transition effort. Timing of this critical step depends on the general contractor and U.S. Army Corps of Engineers (USACE) construction contract completion, building commissioning and other final closeout requirements. Along with these construction-related, time-intensive activities, hospital departmental equipment and personnel moves were also considered. An adaptable agreement for joint-use in overlapping acquisition activities serves as an essential and cost-effective tool to maximize collaboration to reduce time and financial burdens to the program.
WHAT IS A JOINT-USE PLAN?
A joint-use plan is an agreement designed by the most relevant stakeholders, including the U.S. Army Health Facility Planning Agency; VWI International, the initial outfitting and transition contractor; USACE; Clark McCarthy Health Partners II, the general contractor; and William Beaumont Army Medical Center. This agreement is meant to ensure constant coordination of activities in overlapping areas of occupancy and responsibility. It also assures that during joint-use the costs for the construction project and the associated initial outfitting and transition activities are minimized. Furthermore, the work needs to be performed safely with no degradation of quality without disruption of project timelines.
SHAPING THE JOINT-USE PROJECT DELIVERY TEAM
The success of every project is driven by the talent and collaboration of its team members. It is measured by having each stakeholder’s role well defined in advance to set clear understanding of their responsibilities. Here, we’ll describe the most relevant stakeholders in the Fort Bliss Hospital Replacement Project and their associated duties.
Program manager, owner and customer. Program manager is represented by the local program office, working in a dual capacity for both the Health Facility Planning Agency and the Defense Health Agency (DHA) during the design and construction stages of the project. The program office represents the U.S. Army Office of the Surgeon General’s interests and intent in support of local commanders with program life cycle facilitation, coordination, initial outfitting and transition, and oversight of capital investment strategies and initiatives.
Construction manager and contracting agent. Represented by USACE Fort Worth District as the contractual design and construction authority for the government. The district contracting officer or the authorized administrative contracting officer within their appointed authority is the only individual authorized to direct changes to the design or construction contracts.
General contractor. Represented by Clark McCarthy Health Partners II as the firm awarded construction contracts, the general contractor is responsible for providing a quality construction product in accordance with the approved contract documents.
Initial outfitting and transition contractor. Represented by VWI International, which supports the U.S. Army Health Facility Planning Agency in providing total turn-key effort. This type of effort often involves the provision of a complete product or service that is ready for immediate use by the end user or owner. VWI provides initial outfitting support with services such as cradle-to-grave project management, medical equipment planning, comprehensive interior design, artwork, signage, resource protection, information technology, communication systems, procurement, warehousing, delivery, installation, inventory and warranty support that can provide everything needed to meet the mission on the first patient day. Also, VWI offers transition and clinical operation planning services designed to ensure smooth processes to support the patient delivery model.
End-user. Represented by William Beaumont Army Medical Center, which is responsible for organizing a transition committee; determining transition funding; manpower, equipment and training needs; and creating an atmosphere of constructive, enthusiastic involvement in the completion and activation of the new medical center.
WHY JOINT-USE?
Overall, joint-use decreases facility operational cost and minimizes equipment and supply variation while decreasing product consumption and inventory, streamlines staff training and creates opportunity for future cost avoidance and savings. There are benefits from reducing project lead times without sacrificing project content. This adds additional project capacity that will allow the program manager to concentrate on other areas that may require more attention because of their complexity. For such, gaining an understanding of a phased acquisition and delivery process is crucial when early occupancy is needed before the completion of construction and project closeout.
To complete such a task, a phased occupancy plan or a formal joint-use plan is required. The joint-use plan is a co-developed agreement between the general contractor and a government organization or its agent that addresses the period before handover or the beneficial occupancy date. Beneficial occupancy date is the date the customer can expect to receive useful occupancy of the facility or construction work ends for the general contractor. The owner may need to continue administering the final stages of the project construction contract until such completion and the user may begin to occupy all or agreed upon parts of the facility and use it for its intended purpose.
The general contractor maintains full and proper control of, and responsibility for the operations and security of the facility. Prior to the beneficial occupancy date, the general contractor “owns” the building while it is under construction and before the government accepts it. During acquisition, especially for a complex medical facility, many types of equipment require extensive coordination for their delivery and installation prior to beneficial occupancy date. Access, schedule, supervision, custody, safety, security, utility provision, mechanical system access and space use, among other items, must be aligned to avoid conflict. The joint-use plan is developed to ensure that the entire facility can be made operational on schedule and the total time and cost to the owner is minimized for the military construction project and for the associated fit-up. The general contractor will ensure that all identified joint-use spaces meet minimum acceptance criteria, defined via coordination with the owner prior to outfitting.
VALUE ADDED
The joint-use plan document provides all parties a foundational understanding about how a project is being phased as part of a strategic delivery process. This is essential for larger projects with equipment items requiring long lead times and extensive access and utility coordination. The value of planned coordination is for all parties to understand the conditions of project phasing, the physical state of project completion, any special permitting or inspections necessary, documentation needed for fire and life safety and other health concerns necessary for a successful joint-use plan for those designated areas. For all other associated parties and other vendors involved with the project, the joint-use plan serves as the tool to determine how to meet the general contractor’s and owner’s ordinances and policies and to properly plug into the project phasing strategy.
APPLYING LESSONS LEARNED
The program office has been gathering lessons learned from various projects in different stages of construction and transition to take corrective action that has been of increased value during the joint-use coordination effort. The program office has drawn lessons from the repository compiled by USACE and the U.S. Army Health Facility Planning Agency. These documents serve as best practices for medical projects during their initial outfitting and transition period.
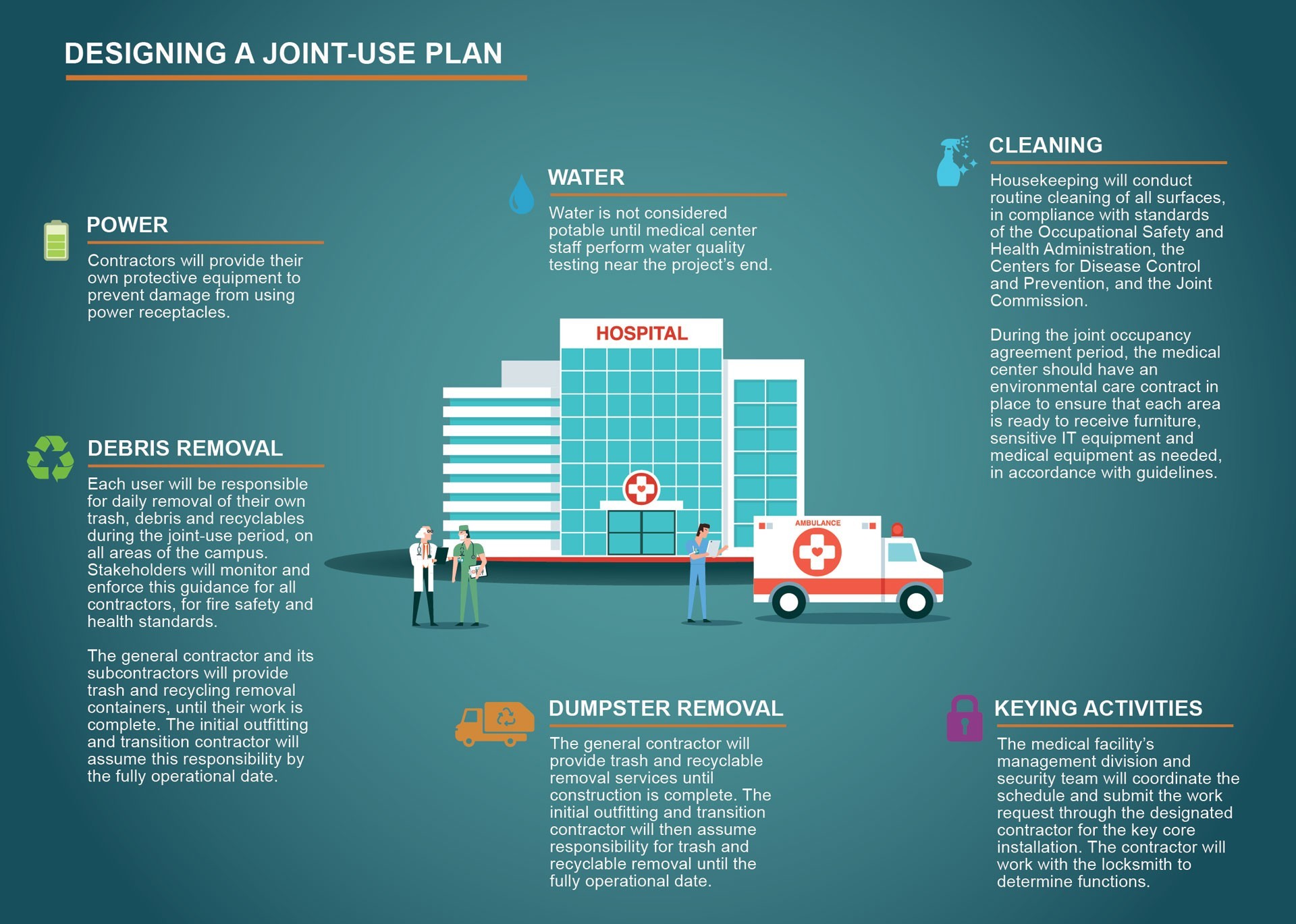
DESIGNING A JOINT-USE PLAN
When planning your project, it is important to involve the end-user and the owner as early as possible so that all parties understand the phasing strategy for both construction and occupancy. Typically, this is done by the project delivery team (architect, engineer, government representatives, agent and contractor). This process is iterative as acquisition proceeds. The initial meeting is most productive when plan review staff and project manager inspection teams are involved, further assuring all parties understand the concept and execution of the phasing plan.

CONCLUSION
Understanding the potential risks and cost overruns associated with transitioning into a new facility can enable the owning organizations to effectively and predictably plan for smooth transitions from construction to operational readiness. Risk mitigation also affects long-term asset management by contributing to lower operation and maintenance costs, increased facility longevity and a superior customer or occupant experience. With an increase in the level of technology in facilities coming online in the near future, it is imperative that the transition planning, workforce preparation and data transference are consistent and reliable for organizations expanding their portfolio and seeking an integrated operation and asset management program from opening day of a new facility. By designing and implementing a carefully constructed and implemented joint-use plan, risks to the owner, agent and the project delivery team are minimized.
COL. EDWIN H. RODRIGUEZ is the program manager for the Fort Bliss Hospital Replacement Project. He has an M.A. in health service management from Webster University and a B.S. in biology from Universidad Interamericana de Puerto Rico. He is health facility planner, supply chain manager and a Lean Six Sigma Green Belt. He is a graduate of Army Command and General Staff College, the Health Facility Planning Agency internship program and the Army Medical Materiel Management internship program.
Read the full article in the Summer 2020 issue of Army AL&T magazine.
Subscribe to Army AL&T - the premiere source of Army acquisition news and information.
Social Sharing