
Great and exciting things are happening in Army Medicine today as we move forward, away from the old Army "healthcare system" to the new Patient-Centered Medical Home "system of health."
As a result of this retooling, a new target has appeared.
"We are committed to finding ways to touch the lives of our patients by promoting individual health and prevention during the time between doctors visits, a time referred to as the "white space," said Army Surgeon General, Lt. Gen. Patricia D. Horoho.
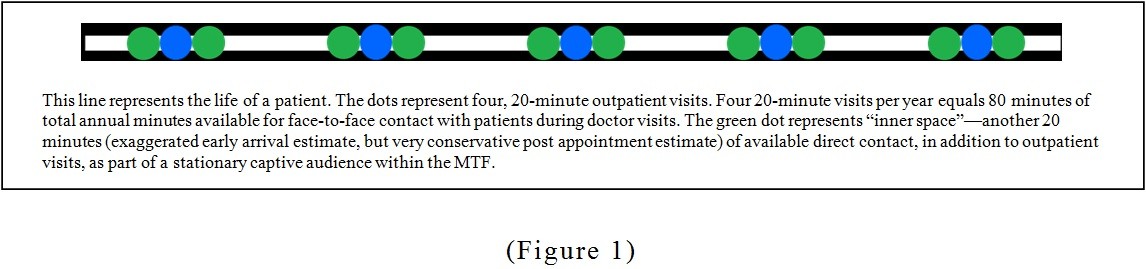
There is an average of 80 hours with patients available for direct individual health promotion and prevention annually, according to Horoho.
But we can easily double that by adding another 20 minutes of "inner space" to each outpatient visit throughout the year.
What's more, we can reach ALL of our seemingly impossible-to-reach target groups within this "inner space" as well.
"Inner space" defined:
Available direct contact, between beneficiaries/potential beneficiaries and the PCMH team, in addition to actual doctor visits.
"Inner space" is white space invaded. This is the holy grail of untapped "white space" where previously unreachable target groups can be found every day--right inside your Military Treatment Facility.
In other words, we could increase the length of time represented by the blue dots in this line by a multiple of two or three, at a bare minimum. But for the sake of argument, let's just double it to 40 minutes per actual doctor visit.
Let's also recognize this additional untapped "space," by looking at it separately from the "outpatient visit" (outpatient visit: that frame of time between entering and exiting a particular clinic).
Each patient concludes his "outpatient visit" not by walking out of the facility, but by taking a number and having a seat in the Pharmacy waiting room for 20 minutes or more.
"Inner space" exists.
Realistically, "inner space" is a far longer span of time than the actual outpatient visit, and is far more valuable in the hands of our professional communicators.
How many potential beneficiaries (those who don't get their care at your MTF) still get their prescriptions filled at your MTF's pharmacy?
The answer: all of them, according to one retiree organization leader I talked with recently.
Let that sink in.
Now, if "inner space" has value to ANY degree, shouldn't we be using it? And shouldn't we be using it properly and effectively as part of our business model?
The Army Surgeon General said we're committed to finding ways to touch the lives of our patients by promoting individual health and prevention "during the time between doctors' visits."
But before your mind goes racing through all of the "inner space" use possibilities, each MTF has a dedicated person, or persons, whose main purpose in life is to communicate command information.
"Inner space" communication is one of their specialties.
MTF Marketing and Public Affairs Office responsibilities
Through the use of your MTF's Qflow system, closed circuit TV, or internal cable channel, your MTF's Marketing Specialist and Public Affairs Officer can reach--and hold--and re-acquire--the attention of these beneficiaries/potential beneficiaries effectively.
Businesses advertise because advertising works. So before you pooh pooh this as not a really monumental idea, consider this:
• Some beneficiaries spend over an hour in a Pharmacy waiting room after an appointment with their healthcare team. What is the value of a 30-second commercial during the Super Bowl? And during the Super Bowl, we're not even a captive audience because we're making a break for the kitchen or the bathroom so we don't miss the game! There are zombies decaying in your Pharmacy waiting room.
• With just four, 90-day prescriptions per year of just one medication, effective use of "inner space" could easily increase re-enrollment of those who have chosen to get their healthcare elsewhere, but still choose to cash-in on the savings of getting their medications here.
But effective communication and marketing is the key.
Command support required
There are some basic, minimum marketing techniques to deploy against "white space" that will require solid command support, as well as updated Rules of Engagement to support our new PCMH "system of health" redirection.
These basic, minimum changes include, but are not limited to:
• Limiting or removing magazines and fliers from MTF waiting rooms. Place them at your MTF's Information Desk and in exam rooms instead.
• Replacing FOX or CNN with a one-hour-long looping video designed to catch and hold--and re-catch--the attention of target groups within the captive audiences (zombies) currently decaying in your waiting rooms. This is a biggie--but absolutely essential to success. *If you support and allow your professional communicators--your Marketing Specialists and Public Affairs Officers--to handle the imminent potential staff and customer outrage that results from switching off CNN and FOX, you will succeed. If not, you will guarantee failure right off the bat.
• We should be happily communicating, educating and even entertaining within our "inner space." Your MTF is a respite from the depressing bad news outside its doors. It is a happy place of healing--a place where like-minded, military-oriented, patriotic, caring people come together as a team (a Patient-Centered Medical Home healthcare team, of which, the patient is a leading member). Your staffs' priority should be to make themselves fully available to patients. They should be encouraged to step out of their comfort zones and unafraid to help patients, just as they imagined themselves doing when they first chose their particular field of healthcare. They chose their medical profession because they care.
• Your MTF should be a place where both staff and patients feel comfortable, welcome, and at home--and they should already view themselves as being on the same team. All communication should stem from that reality.
• Ensure that your communication specialists have full authority to influence the design and content of this video loop, and leading collaborative rights in the operation of the Qflow system, closed circuit TV, or internal cable channel. The Marketing and Public Affairs Office should be your organization's POC for external communications. Period. External communications include everything your organization communicates to the public, or is within public view, both inside and outside the MTF.
• The Marketing and Public Affairs Office can communicate anything to these captive audiences just as effectively within a waiting room, as the rest of your PCMH team can communicate from within an exam room--and in some cases, far more effectively.
Still pooh poohing?
Remember those potential beneficiaries who don't get their care here? You know--those target groups that we want to re-recruit instead of force back to the MTF?
Well, they're sitting in your Pharmacy waiting room right now watching CNN, complaining about having to wait for their meds.
And those who don't get their healthcare or medications filled here--the next best way of reaching them is still the Pharmacy waiting room.
That's because Word Of Mouth (WOM) is the most effective form of advertising.
The next best chance we have, other than communicating with them face-to-face in an exam or waiting room, is in the form of WOM from their friends--who are sitting in your Pharmacy waiting room right now watching CNN, complaining about having to wait for their meds!
Marketing Video Master Loop (MVML) composition
Here are some ways to immediately and efficiently acquire, and hold--and re-acquire--the attention of these captive audiences:
• Provide fresh, continuous, short (optimally, 7-10 seconds), attention-getting video clips of all kinds, all in the form of one very long video product that loops. If you have a patient demographic that waits 90 minutes for meds, your MVML better be 91 minutes long--just in case!
• Your MVML could show a clip of a Primary Care Manager, sitting behind her desk, speaking directly into the camera, reminding patients to take their meds according to the instructions on the bottle. The clip should be 7-to-10-seconds long, and unscripted.
• Next, show a colorful, informative, professional slide with three brief talking points--information a department needs its patients to know. How about providing information that patients want to know?
• Show a team nurse reminding patients to ask their PCMH team about wellness checks.
• Educate about wellness checks with three-bullet slides or short video news-type products.
• Show a nice photo or video clip of a local attraction--this is a great place to be stationed!
• Does your MTF allow therapy dogs? Therapy dogs don't present allergy problems on video!
• Play an appropriate, attention-getting sound bite now and then.
• Ask a question. Provide the answer later in the MVML.
• Present your command messages, in separate segments, in an unscripted manner, using a combination of text, video, audio and graphics. These can appear both canned AND unscripted to reach everyone. Have a child present a command message.
• Smiles, smiles and more smiles. Real smiles. Genuine, unscripted smiles. Your professional communicators know how to draw out smiles from those they're communicating with.
• Throw your Command Video and a MEDCOM video or two into the mix--your MVML needs to be a very long, editable product. Each segment can also be used in many other ways too (Facebook, website, podcast, radio spot, CORE, attached to an on-line Hometown News Release, etc.). The possibilities are only limited by available manpower and budget.
• Show another nice slide with upcoming holiday hours changes--or a video clip of the department chief informing her beneficiaries of these changes.
• Please--no canned Safety Messages! Let your commo pros add some professional pizzazz to any short messages about safety and any other subject that traditionally puts folks to sleep.
• Use professional moving graphics--this is video!
• Show a short still video clip of an attractive, under-used entrance to your facility where you have better parking available, or patients entering/exiting the facility there. Add natural sound like birds chirping.
• Answer rumors and complaints that would be appropriately answered in the MVML.
• Your commo pros can share pertinent Marketing products with other MTFs. They are all part of the great big MEDCOM commo team!
• They will update and rearrange MVML clips monthly, and as they go out of date, at a minimum.
• They know how to breed familiarity through professionalism--but with personality! Your communication specialists know how to do this most effectively. They know what categories of information to hit, and what techniques to use for affect.
This should not be a difficult thing for your average Marketing Specialist or PAO--they're trained and passionate about achieving effective communication.
They can make it happen.
But success, of course, is wholly dependent on your ROE and leadership support of its Marketing/PAO departments.
Senior leader responsibilities
Leaders, if your Marketing and PAO ROE hasn't changed along with your PCMH system recalibration, consider allowing these commo pros to operate 'at the top of their license' just like any other PCMH team member.
Autonomous tactical execution of the annual Strategic Communications Plan that you approved in January will allow your professionals' maximum "white space" target selection and efficient execution.
• Effectively communicating command information, and your unique command messages, is your Marketing Specialist or PAO's job. Provide direction, but trust them. Give them the tools, and give them the autonomy, to take the ball and run with it.
• Tell your leaders and staff, publically, that you trust and support your Marketing Specialist/PAO's efforts. Staff will cooperate better and far more efficiently. It doesn't take much time to shoot 7-10 seconds of video--but it takes forever to get folks to agree to get shot! No one likes to get shot--it's very uncomfortable! But with your triage of direction, this process becomes very quick and easily--even painless! Your Marketing Specialist/PAO is very busy too, so they need to get this done on the fly if possible. The optimum average shoot should be a drive by, or hastily set up meet with a staff member, to facilitate minimum stress and unscripted responses. Five minutes is not an unrealistic timeframe for a shoot of this nature.
• You must ensure that they have the most basic tools, however. Just $3,000.00 will get them a Nikon D600, a professional camera with two good lenses and provide the ability to acquire both still and video in an affordable manner that no other Digital Single Reflex Camera can (has audio monitoring and a variety of both uncompressed and compressed video acquisition formats and live video monitoring right on their laptop. They've got a laptop, right?). The D600 is the one camera that solves many of the focus issues associated with shooting HD video on a DSLR camera, as opposed to having a dedicated, separate and complex $20,000.00+ HD video solution.
• Squeeze $3,000.00 out of your budget. Marketing is a revenue center. You'll be happy you did.
• Even if your budget cannot accommodate basic marketing tools like a professional still or video camera and professional video editing software (another $3,000.00), you can still pass the ball to your marketing specialist/PAO. With your support, and even without a budget, they can find ways to make the impossible possible, professionally. And given autonomy, with your blessing, they'll find the most direct and efficient route to the goal as well.
• You've already approved your Annual Strategic Communication Plan--give your Marketing Specialist/PAO full authority to tactically execute.
• Communication is hard--but your Marketing Specialist or PAO can handle it--that's their job. Don't expect perfection, however, because your concept of perfection will not line up with accepted Marketing and Public Affairs standards. Creativity is essential--and it is essential for you to support your commo pros' efforts. Your support will foster their creativity. Your forgiveness will encourage greatness.
• Autonomy of operation, with a whole new ROE to reflect our new PCMH "healthcare system," is the answer. You may know PCMH, but you do not know the best way to reach a particular target demographic, given this MVML communication method. That's why you have a Marketing Specialist or PAO!
• Commanders--allow your Marketing or Public Affairs department to shoot video of you just saying hi and reminding your retiree beneficiary team members to help themselves to the free coffee and exclusive retiree beneficiary WIFI available in the your MTF's exclusive USO-type retiree beneficiary den area (and say it in 7-10 seconds!). Yep--that's right--why wouldn't you offer a place like that for your most influential and desired pool of potential beneficiaries? How much money will your MTF make by recruiting just one additional beneficiary? Would it pay for all of this special treatment...er...Marketing? How many additional customer-service oriented staff members, Greeters, Marketing Specialists, or Hospitalists could you add to your staff by recruiting a dozen new beneficiaries?
• Leaders, unless you have the time available to fully devote to your unit's communication/Marketing effort--and Marketing is your specialty--ensure your ROE allows your commo pros to execute battlefield decision making. Keep an eye out for their new products and reel them back in if you must, but don't make them get their products approved before they're deployed. This is a fast-paced biz.
Autonomy of operation is the cornerstone of your commo pros' new ROE.
The possibilities are endless if you understand that you don't specialize in Marketing, make the handoff and support your commo pros, and positively encourage creativity.
We advertise because advertising works.
Trouble is, it can be difficult to measure the actual effectiveness of advertising.
And without numerical quantification, a marketing revenue center can seem more like a cost center to leadership. Your commo pros understand that too.
Coupled with a history of Marketing and Public Affairs difficulty at finding a place of recognized value within and among your more traditional special staff, many leaders' evaluation of marketing expenditures as a cost center has become further solidified--something nice to have but not really essential to mission execution.
Budget or not, your Marketing or Public Affairs Office probably already has its sights on ways to knock down your unit's "white space." But they're likely stymied by budget and manpower shortcomings, and still operating under the same old ROE, from the same old Army "healthcare system."
If so, check your headspace and timing--recalibrate!
Your trust and confidence will allow your communications specialists to invade "inner space," acquire new targets, squeeze the trigger, and hit todays new and elusive "white space" targets.
With the right ROE, their marketing mix can even reach the unreachable and both your enrollment and budget will begin to increase.
(Editor's note: John Brooks is the Marketing Specialist and Public Affairs Officer at the General Leonard Wood Army Community Hospital)
Social Sharing